Adolescent Idiopathic Scoliosis (AIS)
What is AIS?
Scoliosis is a structural deformity of the vertebrae (bones) in your spine. This most commonly develops through the growth stages in early adolescent years when bony growth of the vertebra is uneven from front to back and side to side. This creates more wedge shaped bones and is often found in conjunction with hypermobility, a condition that is characterized by excessive joint movements. This blend of bony wedging, hypermobility and associated relative muscle weakness can lead to the development of “C” or “S” shaped curves in the spine and the development of a scoliosis.
How is AIS diagnosed?
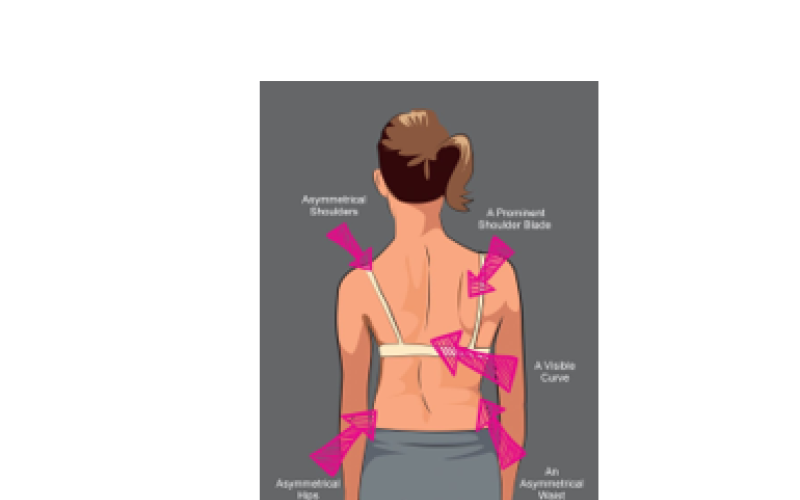
Scoliosis is often first diagnosed when changes in alignment are identified (Figure 1), when prominence of the rib cage is noted with forward bending or if there is pain. Important factors include stage of development (e.g. height, weight, Tanner scale), presence of hypermobility, familial history, and of course, the size and specifics of the curve. Depending on the size of the “hump”, an Xray will be requested that will measure the angle of the curve (Cobb angle), the level of the curve, the shape of the curve and the stage of growth (Risser Grade). This will help the treating health professionals identify the risk for curve progression and determine the most appropriate management.
What are the risks for progression of the curve?
Research suggests that there are two major determinants that help us identify the risk of a scoliotic curve progressing in angle.
These are:
AGE - This relates specifically to age in relation to the growth spurt. It has been demonstrated that the earlier a curve presents, the more chance there is of progression. In females, there is a greater risk to increasing curve size in the period starting the 6 months prior to the onset of menstruation and for 2 years following the first “period”. In males, this is a little later – around the age of 13-14.
SIZE OF THE CURVE - The larger the curve at a younger age, the more chance there is of progression as the adolescent fights to maintain upright posture against gravity.
Other factors that may also contribute to concerns are the presence of hypermobility and concurrent flattening of the thoracic kyphosis/lumbar lordosis that frequently occurs in conjunction with a scoliosis.

Frequently Asked Questions
- How is scoliosis treated?
The management of an adolescent with scoliosis is dependant upon their age, stage of maturity and most importantly, the size of their curve. All diagnosed with scoliosis will need to undertake strengthening and mobility exercises aimed at maintaining posture against gravity. However, for those whose Cobb angle is ³ 25°, bracing will usually be required in order to try to prevent further curve progression and to assist curve reduction. For curves over 60°, surgery is usually recommended to ensure quality of life and general health as an adult.
- Which activities or movements should be avoided?
When exercising, bending forwards / sideways and twisting should be avoided where possible to prevent further curve progression. Sports, such as rowing, cycling and swimming, that require repetitive bending and twisting should also be discouraged because of their impact on the scoliotic spine.
- How does physiotherapy help with the scoliotic spine?
The aim of physiotherapy management is to develop an individualised exercise program that will create a strong, stable scoliotic spine capable of fighting the forces of gravity to maintain a good, upright posture. Physiotherapy can also be useful in treating pain that develops secondary to the scoliosis. Pain is not always a complaint but appears to be more prevalent in the right side when the thoracic kyphosis and/or lumbar lordosis has also flattened in response to changes to the vertebral shape. However, care needs to be taken as pain is usually a result of weakness and stretch rather than tightness, and massage may lead to more pain as the muscles relax and switch “off” instead of working hard to hold the adolescent up against gravity!
- What is the effect of bracing on the scoliotic spine?
For curves over 25°, bracing aims lift up under the armpits and push the hips down to produce gaps between the vertebrae so that the growth plates can develop more normally. The brace also pushes the spine sideways to make is as balanced as possible to further open up the growth plates on the concave side and “squash” the curve slightly on the convex side. This process seeks to allow the vertebrae to develop to be the most structurally optimal shape and in the best position possible. Even though wearers need to use the brace for 22 hours per day, 85% avoid surgery if they are compliant with this regime! It is important to note that there will usually be a persisting 10°+ curve at the end of bracing, but the spine does not need to be straight, just balanced!!


- What are the major concerns of adolescents with scoliosis?
Interestingly, when scoliotic adolescents were interviewed regarding their aims for treatment, usually their main concerns related to stopping the progression of the curve and to improving aesthetics. They also described feelings of anxiety, fear of the unknown (e.g. worried about the curve progressing and how it will look), coping if required to undertake more formal management (e.g. bracing) and pain. For the successful management of these individuals, it is important that they are guided to develop some level of control over these important issues.